The Miller School and the KiDZ Neuroscience Center at The Miami Project to Cure Paralysis held a special assembly at Ransom Everglades School in Coconut Grove this month to educate students about spinal cord injury and concussion in sports.
At the September 13 assembly, Marc Buoniconti, president of The Miami Project to Cure Paralysis, discussed the college football injury that left him paralyzed 25 years ago and the advances in spinal cord injury research, including the start of human trials, that hold promise of a cure.
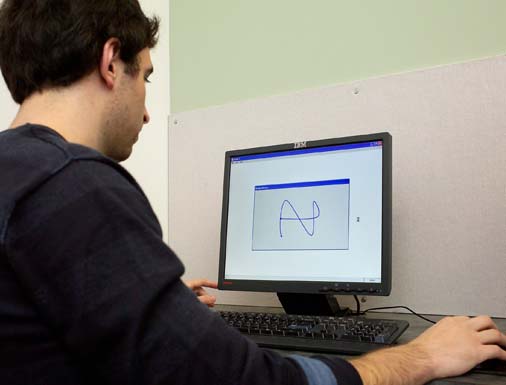
And Gillian Hotz, Ph.D., director of the Concussion Program at UHealth Sports Medicine, reviewed the signs and symptoms of concussion and described how Ransom students will be tested with ImPACT this fall.
A computerized neurocognitive assessment tool, ImPACT is used by coaches, athletic trainers, doctors, and other health professionals to help determine whether athletes are fit to return to play after suffering a concussion. Administered pre-season, the 30-minute test establishes a baseline which can be used to compare to post-injury tests, and to devise the best course of treatment.
Behind Miami Project President Marc Buoniconti, center, are from left, Claude Grubair, athletic director; Adam Goldstein, parent; Ellen Moceri, head of Ransom; David Goldstein, student; Gillian Hotz, Ph.D., and Cheryl Goldstein, parent.
Hotz also introduced David Goldstein, a 10th-grade student who suffered multiple concussions while playing soccer. David described how Hotz and Kester Nedd, D.O., voluntary associate professor of neurology, treated his post concussive symptoms at the UHealth Sports Medicine Concussion Clinic and recommended the return-to-play program under which he gradually improved and was able to resume playing soccer.
David and Ransom are now teaming up to raise money for ImPACT testing for all of Miami-Dade County’s public high school football players starting next spring, and to support the research efforts of the Concussion Program.
UB researchers are the first to show that a controlled individualized exercise training program can bring athletes and others suffering with post-concussion syndrome (PCS) back to the playing field or to their daily activities.
In a paper published in the January issue of the Clinical Journal of Sport Medicine, the researchers report that a program of progressive exercise developed individually for each participant and performed at levels just below the onset of symptoms is safe and can relieve nearly all PCS symptoms.
Their results counter the accepted wisdom that PCS should be treated with rest, reassurance and antidepressants, and that physical activity should be avoided.
“Perhaps the most exciting aspect of this study is that all of the subjects that participated, both athletes and non-athletes, got better eventually, although the athletes certainly improved the fastest,” says Barry Willer, professor of psychiatry and rehabilitation sciences and senior author on the study.
“It also was reassuring to discover that the use of exercise was safe and did not prolong symptoms, a worry expressed by other practitioners.”
John J. Leddy, associate professor of orthopaedics and co-director of UB’s Sports Medicine Institute, where the study was conducted, is first author on the study. Willer, Leddy and Karl Kozlowski, clinical instructor of exercise and nutrition sciences, developed the exercise protocol.
For unknown reasons, 5-10 percent of people who experience a concussion have symptoms that persist beyond six weeks. These persons are diagnosed with PCS. Previously, there was no treatment for the condition with proven success.
The UB regimen is based on the hypothesis that the regulatory system responsible for maintaining cerebral blood flow, which may be dysfunctional in people with a concussion, can be restored to normal by controlled, graded, symptom-free exercise.
The researchers developed their program in 2004. “We were testing athletes for return to sport using an exercise test,” says Willer, “and we decided that if an athlete becomes symptomatic at a heart rate of, say, 140, maybe they could exercise at a heart rate of 125, without complications. We soon discovered that the athletes got better much quicker if they exercised.”
Physicians in UB’s Sports Medicine Concussion Clinic initially used their approach only with athletes from UB teams, but word spread and they now have assessed and treated many professional athletes, especially those from the National Hockey League.
“One of the advantages we offer to professional teams is a more precise test of post-concussion syndrome,” says Leddy. “If the patient does not develop symptoms during the exercise test, then the cause of their difficulties is likely to be another source. Most commonly it is neck strain, which tends to cause headaches that mimic post-concussion headache.”
For the preliminary study just published, the researchers enrolled six non-athletes who suffered concussions in auto accidents or falls, along with six athletes—five who were injured in their sport and one in a car accident.
Participants were tested initially on a treadmill to determine the exercise intensity that triggered symptoms. With individual baselines established, each participant exercised at 80 percent of that intensity every day for three weeks and then returned for a repeat test. In most instances, retesting demonstrated that participants could work at a higher intensity and the exercise protocol then was increased. This pattern continued until participants could exercise completely without experiencing PCS symptoms.
As might be expected, the athletes recovered more quickly than the non-athletes, results showed. They returned to normal within 11 to 36 days, while the non-athletes required 41 to 112 days of intervention. All participants had returned to work, school or athletic activities at a three-month, post-program follow-up.
Ten of the 12 participants were completely free of symptoms at follow-up. One participant still experienced cognitive and visual symptoms, and another, who had a history of migraines, continued to experience headaches.
“The data suggest that some PCS symptoms are related to disturbed cerebral autoregulation, and that after this treatment, the brain was able to regulate blood flow when the blood pressure rose during exercise,” says Leddy. “We think progressive stepwise aerobic training may improve cerebral autoregulation by conditioning the brain to gradually adapt to repetitive mild elevations of systolic blood pressure.”
Kozlowski adds that although each concussion should be considered a “unique injury,” a randomized trial that included a PCS control group should be conducted to address the possibility that PCS symptoms would have resolved spontaneously without intervention.
“All of our subjects had been symptomatic for months before treatment and were not getting better on their own,” says Kozlowski, “so we are pretty convinced that the regulated exercise program did the trick.” A grant application to the National Institutes of Health to conduct such a randomized trial currently is under review.
Also contributing to the study were James P. Donnelly of the Department of Counseling, School and Educational Psychology; David R. Pendergast, professor of physiology and biophysics; and Leonard H. Epstein, professor of pediatrics.
The study received financial support from the Buffalo Sabres Foundation and the Robert Rich Family Foundation.
A high school athlete with a history of three or more concussions who sustains a new concussion may be up to nine times more likely to experience common symptoms compared to high school athletes with no history of concussion, according to a University of Pittsburgh study, published in the November issue of the journal Neurosurgery.
?The study is the first to actually demonstrate what have been the commonly assumed cumulative effects of multiple concussions in high school athletes,? according to lead author Michael W. (Micky) Collins, Ph.D., a neuropsychologist and assistant director of the University of Pittsburgh Center for Sports Medicine?s Concussion Program. ?The study indicates for the first time in the high school athlete population that prior concussions may indeed lower the threshold for subsequent concussion injury and increase symptom severity in even seemingly mild subsequent concussions,? he said.
?Our findings are significant because high school athletes in contact sports are at high risk for repeated concussions, yet it is a population that has been understudied regarding concussion management,? Dr. Collins said. ?Quite often the athlete?s concussion history has weighed heavily in the return-to-play decision process, although this has been based on little scientific data. Our findings highlight the need for more long-term outcome studies in this population.?
Concussion symptoms are not always reported by the athlete and the effects are difficult to objectively measure. Thus, the determination of when it is safe to return an athlete to play is not always straightforward, according to Dr. Collins. Previous research has shown that allowing enough time for the brain to heal and recover before return-to-play is crucial in preventing more severe damage from possible further brain trauma during contact play. Generally, he said, most athletes who sustain an initial concussion can recover completely as long as they are not returned to contact sports too soon.
More than 10 percent of high school athletes participating in contact sports in the United States sustain a concussion each season, according to previous studies. A concussion can occur when the brain is violently rocked back and forth inside the skull due to a blow to the head or upper body. A concussion is a trauma-induced alteration of mental status that may or may not result in loss of consciousness. Other symptoms may include disorientation, confusion, dizziness, amnesia and uncoordinated hand-eye movements.
Dr. Collins? team investigated 88 high school athletes who sustained concussions during the 2000-2001 school year and were evaluated as patients of the University of Pittsburgh Center for Sports Medicine?s Concussion Program. Sixty athletes with no prior concussion history were compared to 28 athletes with a history of three or more concussions. The two groups were compared in terms of on-the-field presentation of four concussion severity markers following an in-study concussion. The symptom markers measured involved loss of consciousness, anterograde amnesia (loss of memory of events after injury), retrograde amnesia (loss of memory of events before injury), and confusion.
Compared to the group with no concussion history, the group of athletes with three or more concussions were nine times more likely to experience three out of the four on-the-field severity markers ? loss of consciousness, anterograde amnesia, and confusion.
Addressing the severity markers specifically: The group with a history of three or more concussions were more than six times more likely to experience loss of consciousness; nearly four times more likely to have anterograde amnesia; and four times more likely to be confused. The odds ratio of retrograde amnesia between the two groups was not significant.
Athletes who participated in the study were from high schools in Pennsylvania, Michigan, Illinois, Oregon and Maine. Among the group with no prior concussion history, 92 percent were males and the average age was 15.8 years. Seventy-eight percent were football players, 8 percent were soccer players, and 5 percent were basketball players. A very small percentage of the group participated in baseball, ice hockey, lacrosse, cheerleading and wrestling, collectively. Among the group with concussion history, 82 percent were males and the average age was 16.1 years. Fifty-four percent played football, 18 percent played soccer, and a very small percentage of the group played basketball, ice hockey, lacrosse, wrestling and volleyball.
Other study authors are: Mark R. Lovell, Ph.D., director of the University of Pittsburgh Center for Sports Medicine?s Concussion Program; Grant L. Iverson, Ph.D., University of British Columbia; Robert Cantu, M.D., Emerson Hospital, Concord, Mass.; Joseph Maroon, M.D., and Melvin Field, M.D., both of the department of neurological surgery, University of Pittsburgh School of Medicine.
The University of Pittsburgh Center for Sports Medicine?s Concussion Program focuses on diagnosis and management of sports-related concussions in athletes of all levels. The program?s internationally-known team of clinicians and researchers are leaders in studying the neurocognitive effects of sports-related concussions and developing better methods of post-concussion evaluation to determine when it is safe for an athlete to return to sports. One method the team has developed is ImPACT (Immediate Post-concussion Assessment and Cognitive Testing). Used worldwide, ImPACT is the first computerized testing system to evaluate the severity of concussions in athletes.
Several problems can occur when a player heads the soccer ball. European players coined the phrase “footballer’s migraine” to describe headaches and some players complain of neck pain and dizziness as a result of heading the ball.
In reality, there is a low occurrence of concussions and other head injuries caused by heading the ball in soccer. Problems are rarely seen in players up to the age of 10 because they don’t try to head the ball very often. However, some problems do occur in older players who are more involved in head ball shots.
A number of studies have been conducted to determine if there is any cumulative trauma from heading the ball in soccer. These studies involve older players and players who have finished their soccer careers. Medical tests, such as the electroencephalogram (EEG), computed axial tomography (CAT scan), and magnetic resonance imaging (MRI), have shown minor physical changes in the brain, and psychological tests in some of these athletes have shown some changes in memory functions later in life. Fortunately, minimal trauma occurs in properly heading the ball. Studies show that the impact is only 20% of that obtained from a boxer’s punch to an opponent’s head.
Improper technique is one of the major causes of injury in heading the ball. Another factor has almost been eliminated with improved equipment. Originally, soccer balls were made of leather and held water. Wet playing conditions created a heavier ball to hit with the head. Modern balls are impervious (non absorbent) to water, thus eliminating the problem. Actually, most soccer related concussions are not related to heading the ball. Rather, they occur when a player is accidentally hit in the head with a ball or has other contact, such as impact with a goal post, the ground, or another player.
Preventive measures can be taken to decrease the risk of injuries with heading a ball. The most important is using proper technique. The head should be stabilized by using the neck muscles, and ball contact should be made with the forehead. Exercises to strengthen neck muscles are important in developing this skill. In the actual head shot, the torso and the head should be aligned with the trajectory of the ball when it is hit. In other words, the player should try to prevent rotation and angular motions of the head and neck while heading a ball. Another prevention factor is enforcement of the rules of the game, particularly encroachment. The distraction caused by this violation may prevent a player from executing the proper technique of heading.
If a player is injured and has symptoms such as headaches, neck pain, or dizziness he or she should be evaluated by a medical professional before resuming play. There has been some discussion of devising headgear for soccer players, but there are concerns the headgear itself may become a source of injury or alter the technique of the game of soccer.
Injuries from heading a ball in soccer are rare and definitely are not a significant problem in the youth age group. For the more advanced player, proper technique and conditioning can keep the risks of head injuries to a minimum.